
Burnout: Causes, Effects, and Coping Strategies
Burnout is a significant problem, not only for the individual experiencing it but also for their family and workplace productivity. Therefore, reducing burnout symptoms or preventing burnout is essential. However, many people with burnout face challenges such as high workloads, low job control, long hours, and work-to-family conflict, which make it difficult to seek professional help. In some cases, structured self-guided adjustments can significantly reduce symptoms
An individual effectively coping with burnout learns to set healthy boundaries, communicates clearly at home and work, prioritizes their own needs, and develops the ability to put challenges into perspective. As a result, their quality of life improves significantly. This guide focuses on reducing burnout symptoms by addressing its most common causes.
This article was written and clinically reviewed by Niels Barends, MSc, licensed psychologist and founder of Barends Psychology Practice. The information is based on current scientific literature and over a decade of clinical experience working with stress- and burnout-related complaints.
Burnout is not a sign of weakness or lack of resilience. In clinical practice, it often develops gradually when high responsibility and sustained stress are combined with insufficient recovery. Early recognition significantly improves recovery speed.
If you are experiencing severe exhaustion, panic symptoms, depressive thoughts, or thoughts of self-harm, please seek professional support promptly. In an emergency, contact local emergency services.
Feeling exhausted, detached, or overwhelmed?
Burnout symptoms can improve significantly with structured support. We offer evidence-based treatment focused on restoring energy, boundaries, and sustainable performance.
All consultations are confidential and conducted by professionals.
On this page
Coping with burnout – common causes
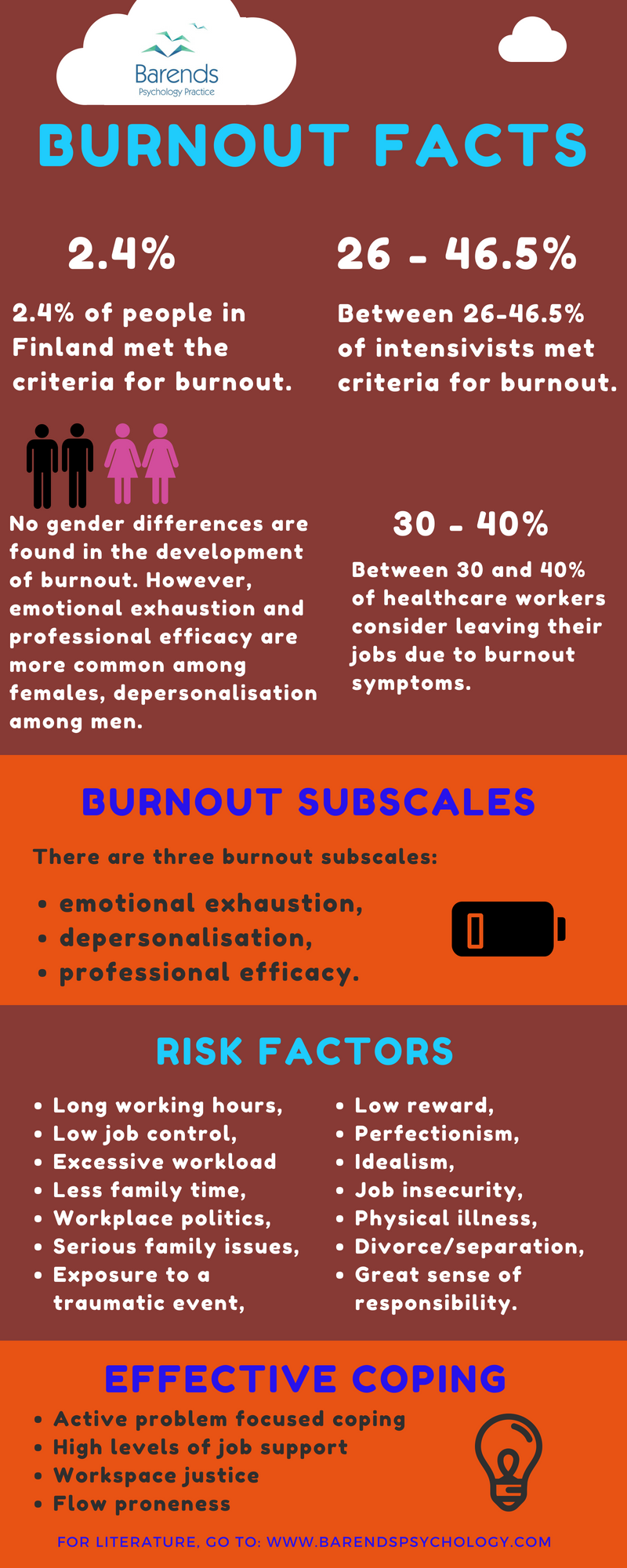
Burnout is divided into three primary subscales, which help explain its complexity:
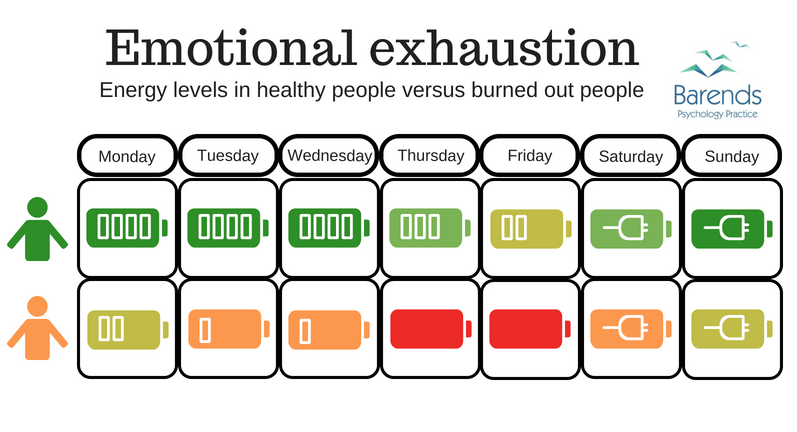
1. Emotional Exhaustion: This is characterized by a lack of energy and an inability to recharge, often leading to feelings of extreme fatigue and being drained [2].
2. Depersonalization: Marked by a distorted view of oneself, others, and the environment, this subscale often results in a lack of empathy, loss of motivation, and feelings of isolation [2],[13],[14].
3. Reduced Professional Efficacy: This includes difficulty concentrating, a negative attitude toward tasks, and a lack of creativity, which can make daily responsibilities feel overwhelming.
Interestingly, an individual doesn’t need high scores in all three areas to be considered burned out. Instead, different causes may uniquely affect each subscale.
Clinically, emotional exhaustion is usually the first signal. If not addressed, it often progresses into cynicism (depersonalization) and eventually reduced professional efficacy. Intervening early prevents this downward spiral.
Common Causes of Burnout
Burnout is typically the result of a combination of factors, rather than a single issue. These include:
• Long working hours [3]
• High workloads [3],[4],[5],[6]
• Low job control [7],[8]
• Organizational fairness [9]
• Work-to-family conflict [10]
• Experiencing traumatic events [11]
• Leadership styles [15],[16]
By identifying these causes, individuals can begin to address their burnout effectively.
(Advertisement. For more burnout treatment information, continue reading).
What can you do to reduce burnout?
Coping with burnout
Coping with burnout is most effective when approached step by step. For instance, focusing on reducing the causes of stress one at a time can make the process more manageable and sustainable.
In therapy, we often focus first on recovery behaviors (sleep, boundaries) before tackling deeper cognitive or organizational issues. Restoring physiological recovery capacity is usually the first step.
Coping Based on Your Stress Pattern
Personality structure influences how stress accumulates and how recovery should be structured. The patterns below are informed by applied personality research and executive performance psychology.
Although workload and organizational factors play a major role in burnout, individual stress responses differ significantly. Some people deplete cognitively, others emotionally, and others physically. The strategies below may therefore feel more or less natural depending on your underlying stress pattern.
Visionary
Visionaries benefit from reconnecting with meaning and long-term direction. Clarifying purpose often reduces emotional exhaustion more effectively than simply reducing tasks.
Strategist
Strategists benefit from reducing cognitive overload and softening internal performance standards. Scheduled mental detachment from work is often necessary, not optional.
Architect
Architects benefit from gradual emotional re-engagement and structured reflection. Sharing strain earlier can prevent prolonged internal overload.
Operator
Operators benefit from restoring physical recovery first. Sleep, breaks, and realistic pacing are often more effective than additional productivity strategies.
Connector
Connectors benefit from boundary clarification and redistribution of emotional responsibility. Learning to tolerate short-term relational discomfort can reduce long-term exhaustion.
1. Working Hours
First and foremost, reducing working hours has been shown to lower burnout rates significantly [12]. This can involve sticking to official work hours, setting boundaries, and creating routines to manage the workday efficiently. For example, preparing for the end of the workday helps reduce stress and ensures tasks are completed on time. Additionally, routines provide structure, which can make it easier to maintain a healthy work-life balance.
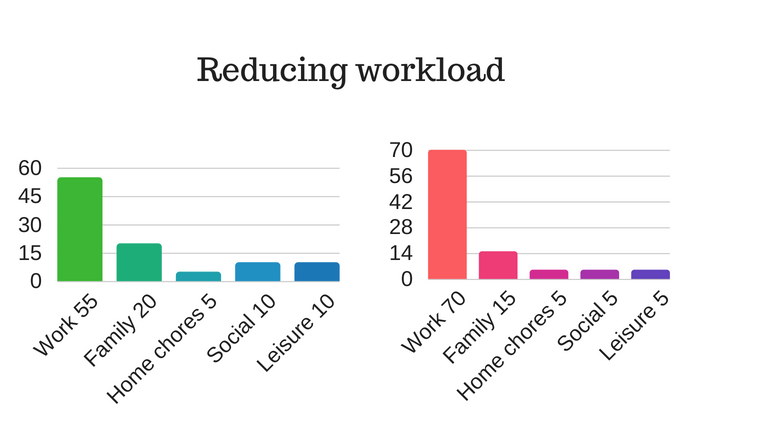
2. High Workloads
A heavy workload increases stress, fatigue, and the likelihood of mistakes [10]. To manage this:
• Slow down productivity: Taking short breaks, allowing more time for tasks, and delaying communication about completed tasks can give you space to recharge.
• Create an energy chart: Tracking weekly activities helps identify where energy is spent. Adjusting the balance between work and personal life can lead to better recovery.
• Ask for help: Delegating tasks reduces stress and creates time for recovery.
3. Low Job Control
Next, improving job control can reduce emotional exhaustion and increase professional efficacy [6],[7]. Strategies include establishing routines and advocating for flexibility in task management or scheduling.
4. Organizational Fairness
While improving organizational fairness may seem daunting, it can significantly reduce burnout. Scheduling a meeting with your supervisor to discuss clear guidelines and regular feedback can foster a more supportive environment [9]. However, proceed cautiously, as changing organizational culture can be challenging.
(Advertisement. For more burnout treatment information, continue reading).
5. Work-to-Family Conflict
Furthermore, reducing work-to-family conflict involves clear communication with your partner and honoring commitments. For instance, prioritizing family over work and keeping your partner informed about deadlines and events can minimize stress and frustration.
6. Traumatic Events
If trauma contributes to burnout, addressing it is crucial. Reaching out to a professional specializing in trauma or PTSD treatment is essential for effective recovery.
7. Leadership Styles
Finally, democratic and transformational leadership styles, which emphasize employee input, encouragement, and rewards, are the most effective in reducing burnout [9]. These approaches increase job satisfaction and engagement, making them beneficial for both employees and organizations.
Final Thoughts
In summary, coping with burnout requires a step-by-step approach that addresses its underlying causes. By making gradual changes to workload, communication, and organizational practices, individuals can significantly reduce burnout symptoms. Moreover, seeking professional support can help tackle persistent challenges, ensuring long-term well-being and resilience.
Frequently Asked Questions about Burnout
How long does burnout recovery take?
Recovery time varies depending on severity, duration, and work conditions. Mild burnout may improve within weeks when recovery behaviors are implemented consistently. More severe cases can take several months and may require professional support.
Is burnout the same as depression?
Burnout is work-related and primarily characterized by exhaustion and reduced professional efficacy. Depression affects multiple life domains and includes persistent low mood, loss of interest, and broader cognitive symptoms. The two can overlap but are not identical.
Can burnout resolve without therapy?
Mild cases can improve with structured recovery strategies, boundary setting, and workload adjustments. If symptoms persist, worsen, or spread into other life areas, professional intervention is recommended.
Coping with burnout – Literature
- [1] INTeReSTS, D. O. (2015). Burnout in physicians. JR Coll Physicians Edinb, 45, 104-7.
- [2] Gorter, R., Freeman, R., Hammen, S., Murtomaa, H., Blinkhorn, A., & Humphris G. (2008). Psychological stress and health in undergraduate dental students: fifth year outcomes compared with first year baseline results from five European dental schools. Eur J Dent Educ., 12, 61–68.
- [3] Van Droogenbroeck, F., Spruyt, B., & Vanroelen, C. (2014). Burnout among senior teachers: Investigating the role of workload and interpersonal relationships at work. Teaching and Teacher Education, 43, 99-109.
- [4] Greenglass, E. R., Burke, R. J., & Fiksenbaum, L. (2001). Workload and burnout in nurses. Journal of community & applied social psychology, 11, 211-215.
- [5] Wen, J., Cheng, Y., Hu, X., Yuan, P., Hao, T., & Shi, Y. (2016). Workload, burnout, and medical mistakes among physicians in China: A cross-sectional study. Bioscience trends, 10, 27-33.
- [6] Salanova, M., Peiró, J. M., & Schaufeli, W. B. (2002). Self-efficacy specificity and burnout among information technology workers: An extension of the job demand-control model. European Journal of work and organizational psychology, 11, 1-25.
- [7] Lourel, M., Abdellaoui, S., Chevaleyre, S., Paltrier, M., & Gana, K. (2008). Relationships between psychological job demands, job control and burnout among firefighters. North American Journal of Psychology, 10, 489-496.
- [8] Hätinen, M., Kinnunen, U., Pekkonen, M., & Kalimo, R. (2007). Comparing two burnout interventions: Perceived job control mediates decreases in burnout. International Journal of Stress Management, 14, 227.
- [9] Greco, P., Laschinger, H. K. S., & Wong, C. (2006). Leader empowering behaviours, staff nurse empowerment and work engagement/burnout. Nursing Leadership, 41-56.
- [10] Wang, Y., Chang, Y., Fu, J., & Wang, L. (2012). Work-family conflict and burnout among Chinese female nurses: the mediating effect of psychological capital. BMC public health, 12, 915.
- [11] Katsavouni, F., Bebetsos, E., Malliou, P., & Beneka, A. (2015). The relationship between burnout, PTSD symptoms and injuries in firefighters. Occupational medicine, 66, 32-37.
- [12] Martini, S., Arfken, C. L., & Balon, R. (2006). Comparison of burnout among medical residents before and after the implementation of work hours limits. Academic Psychiatry, 30, 352-355.
- [13] Michal, M., Sann, U., Niebecker, M., Lazanowsky, C., Kernhof, K., Aurich, S., … & Berrios, G. E. (2004). Die Erfassung des Depersonalisations-Derealisations-Syndroms mit der Deutschen Version der Cambridge Depersonalisation Scale (CDS). PPmP-Psychotherapie· Psychosomatik· Medizinische Psychologie, 54, 367-374.
- [14] Eckhardt-Henn, A. (2004). Dissoziative Störungen des Bewusstseins. Psychotherapeut, 49, 55-66.
- [15] Harms, P. D., Credé, M., Tynan, M., Leon, M., & Jeung, W. (2017). Leadership and stress: A meta-analytic review. The Leadership Quarterly, 28, 178-194.
- [16] Schyns, B., & Schilling, J. (2013). How bad are the effects of bad leaders? A meta-analysis of destructive leadership and its outcomes. The Leadership Quarterly, 24(1), 138-158.