
Why do people develop somatic symptom disorder?
Somatic symptom disorder facts
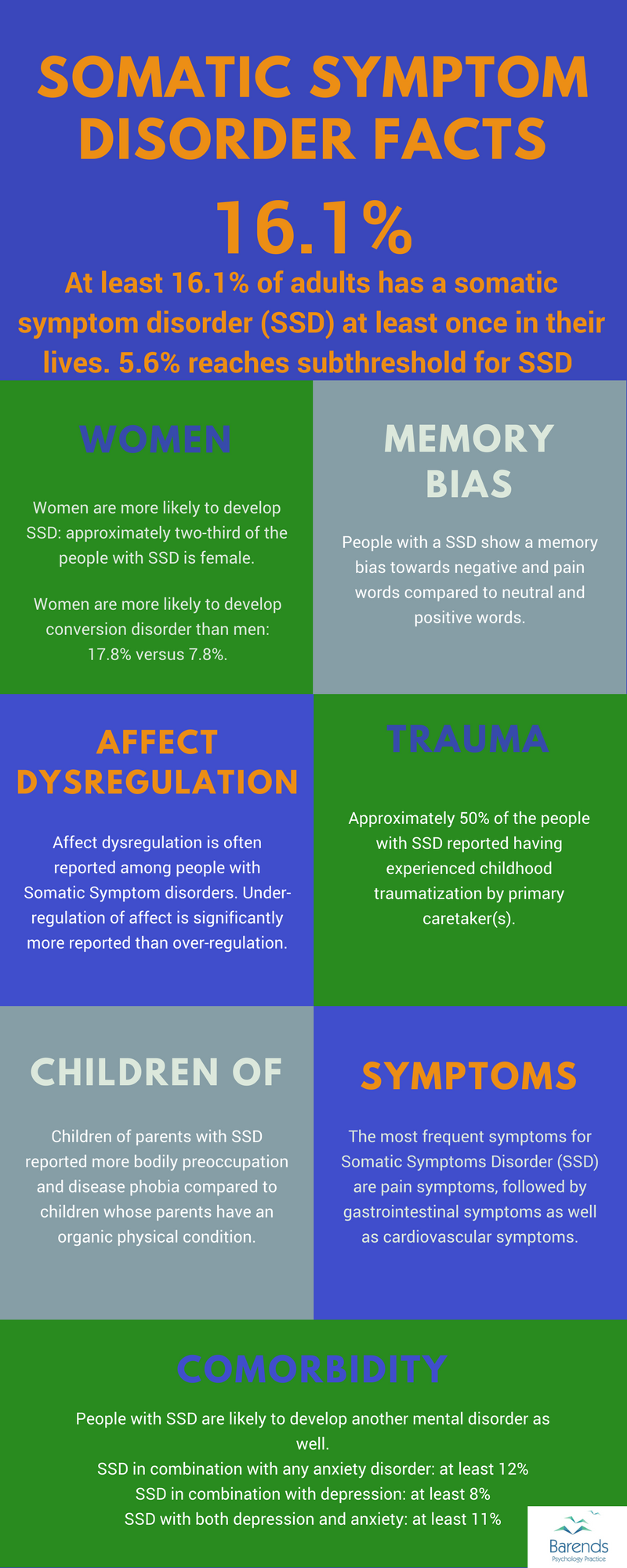
Around 16% of people develops a somatic symptom disorder (SSD) at least once in their lives [1],[2],[3]; 5.6% reaches subthreshold SSD in particular [2]. An interesting question to answer is: what are the somatic symptom disorder causes? Have these people inherited certain genes that explain (some) of their SSD symptoms or does the way they have been raised explain why people develop SSD in time? Perhaps something traumatic triggered the development of SSD… Of course, the answers to these questions create new questions, such as: if there is a genetical component, does that mean that everyone who carries it will develop SSD?
This page focuses on these questions and tries to find answers for all of them using scientific literature. This page also offers tools to prevent some somatic symptom disorder causes to affect someone’s life or at least reduce its impact.
NOTE: please be aware that most scientific research has been conducted using the DSM IV definition of somatoform disorders. Somatic Symptom disorder is a new name for the adjusted somatization disorder. For more information about it, please go to: somatic symptom disorder.
Jump to:
At Barends Psychology Practice, we offer (online) therapy for somatic symptom disorder. Contact us to schedule a first, free of charge, online session. (Depending on your health insurance, treatment may be reimbursed).
Somatic symptom disorder causes – genetics
In two neuroendocrine systems associations between somatic symptoms and genetic variation are reported; the serotoninergic system and HPA axis [5]. The serotoninergic system is important in suppressing certain responses; the HPA axis is important for the stress reaction. If the serotoninergic system does not work properly, someone could respond more often to triggers/stimuli from its environment. The HPA axis responds to the serotoninergic system. Both can add in this way to the development of somatic symptom disorder symptoms. These associations could not be explained by the co-morbid depression and anxiety symptoms [5].
Neuroticism is a risk factor for developing somatic symptom disorder; one third of the genetic variance in somatic distress could be explained by one common factor: the susceptibility to psychological distress (the tendency to respond to situations with fear, sadness, embarrassment, anger, guilt, and disgust) [7], which is a different way to describe neuroticism. On top of that, neuroticism is related to a self- or body-focused disposition. Another common genetic factor has been associated with somatic distress; this factor accounts for more than 30% of the genetic variance [7].
Somatic symptom disorder causes – environment
Children raised by parents with somatoform disorders are more preoccupied with their body and score higher on the disease phobia scale, compared to children of parents without this mental disorder [8]. Also, they had similar beliefs about their health as their parents [8].
Students report more somatization symptoms if they come from a dysfunctional family [9]. Children of fathers (not mothers) who show more hostility and/or rejection towards their children report more often somatic symptoms than children from a healthy family [10],[11]. Also, the likelihood of developing somatic symptom disorder increases if the parents are negligent/indifferent towards their children [11].
Somatic symptom disorder causes – traumatic experiences
Post-traumatic stress disorder is a good predictor for developing somatic symptom disorder [12]. Approximately 50% of the people diagnosed with somatic symptom disorder has experienced childhood traumatization by the primary caretaker [13]. Also, experiencing traumatic events increases the reported SSD symptoms significantly [14].
67.8% of the people diagnosed with SSD reported any severe trauma [15], however, there is no statistically significant association between sexual abuse and a diagnosis of somatoform disorders [6],[9].
(Advertisement, please scroll down for more facts)
Somatic symptom disorder causes – summary and answers
Based on the above mentioned articles, the somatic symptom disorder causes are genetics, environment, and experiencing traumatic experiences. Inheriting certain genes does not mean that someone will develop SSD, and experiencing a traumatic event does not mean someone will develop SSD. It does, however, increase the likelihood of someone developing somatic symptom disorder.
Parenting styles have a significant impact on children and adolescents. Rejecting/neglecting a child does not only increase the likelihood of developing SSD, but can also lead to several other mental disorders (narcissistic personality disorder & borderline personality disorder, for instance). On top of that, children tend to adopt their parents beliefs, which also significantly increases the likelihood of developing SSD. Therefor, one of the most important things to do for parents, is to be aware of the impact their own behaviour has on their children.
If you notice your child develops somatic symptom disorder symptoms or PTSD, please schedule an appointment with a mental healthcare professional.
If you are traumatized yourself and notice you are suffering from somatic symptoms disorder symptoms, please consider reaching out to a mental healthcare professional, because there are evidence based treatments available for you.
Literature
- [1] De Waal, M. W., Arnold, I. A., Eekhof, J. A., & Van Hemert, A. M. (2004). Somatoform disorders in general practice. The British Journal of Psychiatry, 184, 470-476.
- [2] Jacobi, F., Wittchen, H. U., Hölting, C., Höfler, M., Pfister, H., Müller, N., & Lieb, R. (2004). Prevalence, co-morbidity and correlates of mental disorders in the general population: results from the German Health Interview and Examination Survey (GHS). Psychological medicine, 34, 597-611.
- [3] Becker, S., Al Zaid, K., & Al Faris, E. (2002). Screening for somatization and depression in Saudi Arabia: a validation study of the PHQ in primary care. The International Journal of Psychiatry in Medicine, 32, 271-283.
- [4] Kendler, K. S., Aggen, S. H., Knudsen, G. P., Røysamb, E., Neale, M. C., & Reichborn-Kjennerud, T. (2011). The structure of genetic and environmental risk factors for syndromal and subsyndromal common DSM-IV axis I and all axis II disorders. American Journal of Psychiatry, 168, 29-39.
- [5] Holliday, K. L., Macfarlane, G. J., Nicholl, B. I., Creed, F., Thomson, W., & McBeth, J. (2010). Genetic variation in neuroendocrine genes associates with somatic symptoms in the general population: results from the EPIFUND study. Journal of psychosomatic research, 68, 469-474.
- [6] Chen, L. P., Murad, M. H., Paras, M. L., Colbenson, K. M., Sattler, A. L., Goranson, E. N., … & Zirakzadeh, A. (2010, July). Sexual abuse and lifetime diagnosis of psychiatric disorders: systematic review and meta-analysis. In Mayo Clinic Proceedings (Vol. 85, No. 7, pp. 618-629). Elsevier.
- [7] Hansell, N. K., Wright, M. J., Medland, S. E., Davenport, T. A., Wray, N. R., Martin, N. G., & Hickie, I. B. (2012). Genetic co-morbidity between neuroticism, anxiety/depression and somatic distress in a population sample of adolescent and young adult twins. Psychological medicine, 42, 1249-1260.
- [8] Marshall, T., Jones, D. P., Ramchandani, P. G., Stein, A., & Bass, C. (2007). Intergenerational transmission of health beliefs in somatoform disorders. The British Journal of Psychiatry, 191(5), 449-450.
- [9] Ghamari, M. (2012). Family function and depression, anxiety, and somatization among college students. Int. J. Acad. Res. Business Soc. Sci, 2, 101-105.
- [10] Lackner, J. M., Gudleski, G. D., & Blanchard, E. B. (2004). Beyond abuse: the association among parenting style, abdominal pain, and somatization in IBS patients. Behaviour research and therapy, 42, 41-56.
- [11] Krishnan, V., Sood, M., & Chadda, R. K. (2013). Caregiver burden and disability in somatization disorder. Journal of psychosomatic research, 75, 376-380.
- [12] Escalona, R., Achilles, G., Waitzkin, H., & Yager, J. (2004). PTSD and somatization in women treated at a VA primary care clinic. Psychosomatics, 45, 291-296.
- [13] Annemiek van, D., Julian D, F., Onno van der, H., Maarten JM, V. S., Peter GM, V. D. H., & Martina, B. (2011). Childhood traumatization by primary caretaker and affect dysregulation in patients with borderline personality disorder and somatoform disorder. European Journal of Psychotraumatology, 2, 5628.
- [14] Killgore, W. D., Stetz, M. C., Castro, C. A., & Hoge, C. W. (2006). The effects of prior combat experience on the expression of somatic and affective symptoms in deploying soldiers. Journal of Psychosomatic Research, 60, 379-385.
- [15] Sack, M., Lahmann, C., Jaeger, B., & Henningsen, P. (2007). Trauma prevalence and somatoform symptoms: are there specific somatoform symptoms related to traumatic experiences?.
- The Journal of nervous and mental disease, 195,
928-933.