
Somatic symptom disorder facts
Somatic symptom disorder facts
Somatic symptom disorder (SSD), formerly known as somatization disorder, is a mental disorder where physical symptoms cannot be explained fully by a general medical condition or by the direct effect of a substance, and are not attributable to another mental disorder.
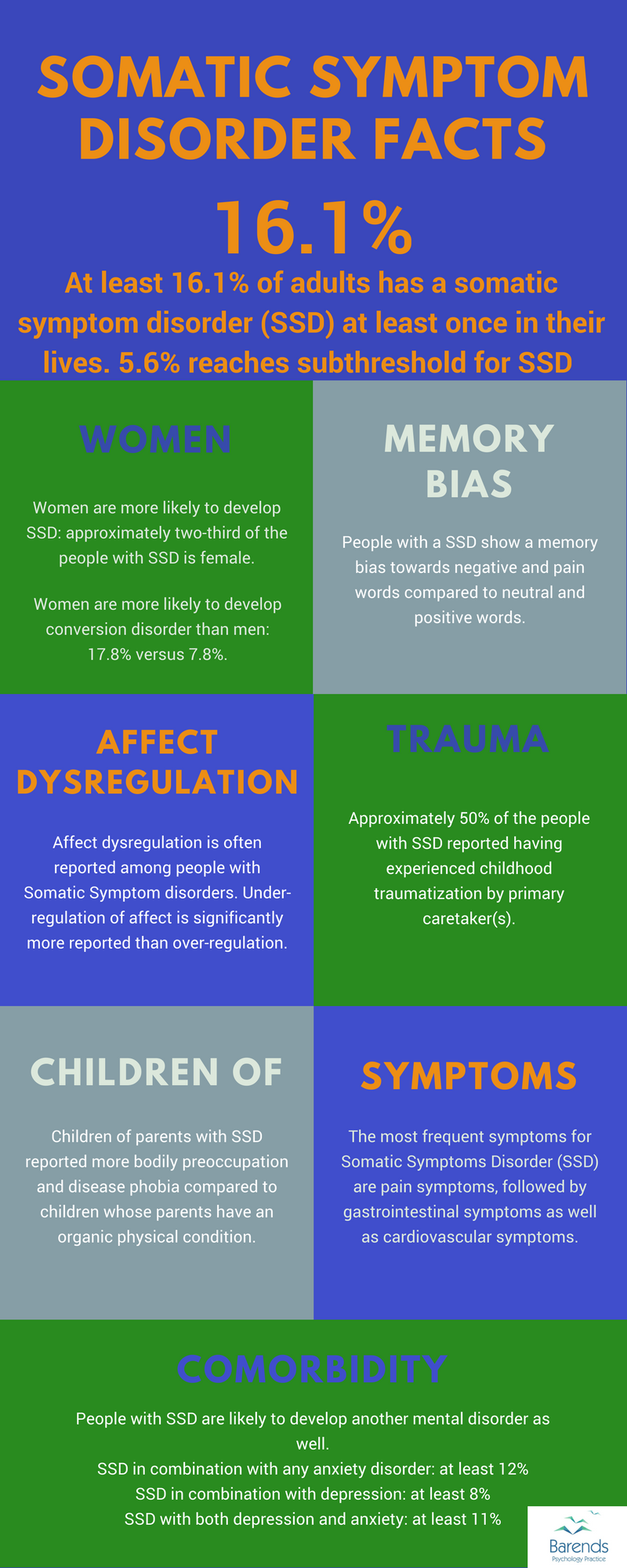
This page discusses scientific somatic symptom disorder facts regarding its prevalence, symptoms, comorbidity, and treatment. One in six people will be diagnosed with SSD at least once in their lives, women are more likely to develop this disorder, and it usually develops around the age of 20. One in two people with SSD report childhood traumatization by primary caretaker(s), is one of the other interesting somatic symptom disorder facts.
Due to the recent publication of the DSM V (published in 2013) and the changed status (name and categorization) somatoform disorders, little research has been done on the new term somatic symptom disorder. That is why this page uses scientific studies about somatoform disorders from 2000 and older. Whenever there is a new publication with Somatic symptom disorder facts this page will be updated.
Jump to:
At Barends Psychology Practice, we offer (online) therapy for somatic symptom disorder. Contact us to schedule a first, free of charge, online session. (Depending on your health insurance, treatment may be reimbursed).
Somatic symptom disorder facts: general information
- People diagnosed with Somatic Symptom disorder (SSD) were more likely to develop another mental disorder in the past 12 months. Mood, anxiety, and other somatic disorders were most prevalent [10].
- People with a SSD show a memory bias towards negative and pain words compared to neutral and positive words [3]. This suggests that the bias is specific to material relevant for this disorder and helps explain why people develop Somatic Symptom Disorders.
- Affect dysregulation is often reported among people with Somatic Symptom disorders. Under-regulation of affect is significantly more reported than over-regulation [5]. In other words, people with SSD have difficulty regulating their emotional state. They tend to regulate their emotional state too little, which explains why they have so many physical symptoms.
- Approximately 50% of the people with SSD reported having experienced childhood traumatization by primary caretaker(s) (TPC) [6]. In case of SSD + Borderline Personality Disorder 75% of the people reported childhood TPC [6].
- Children of parents with SSD reported more bodily preoccupation and disease phobia compared to children whose parents have an organic physical condition [7]. This suggests that these children are more likely to develop a SSD themselves.
- Deafness, erectile dysfunction, loss of memory, joint pain, pain in extremities, palpitation, or urological problems are more common in people aged 45 and older [11].
- Hypochondrical symptoms are more common in people aged 45 and older [11].
Somatic symptom disorder facts: symptoms
Somatic symptom disorder symptoms
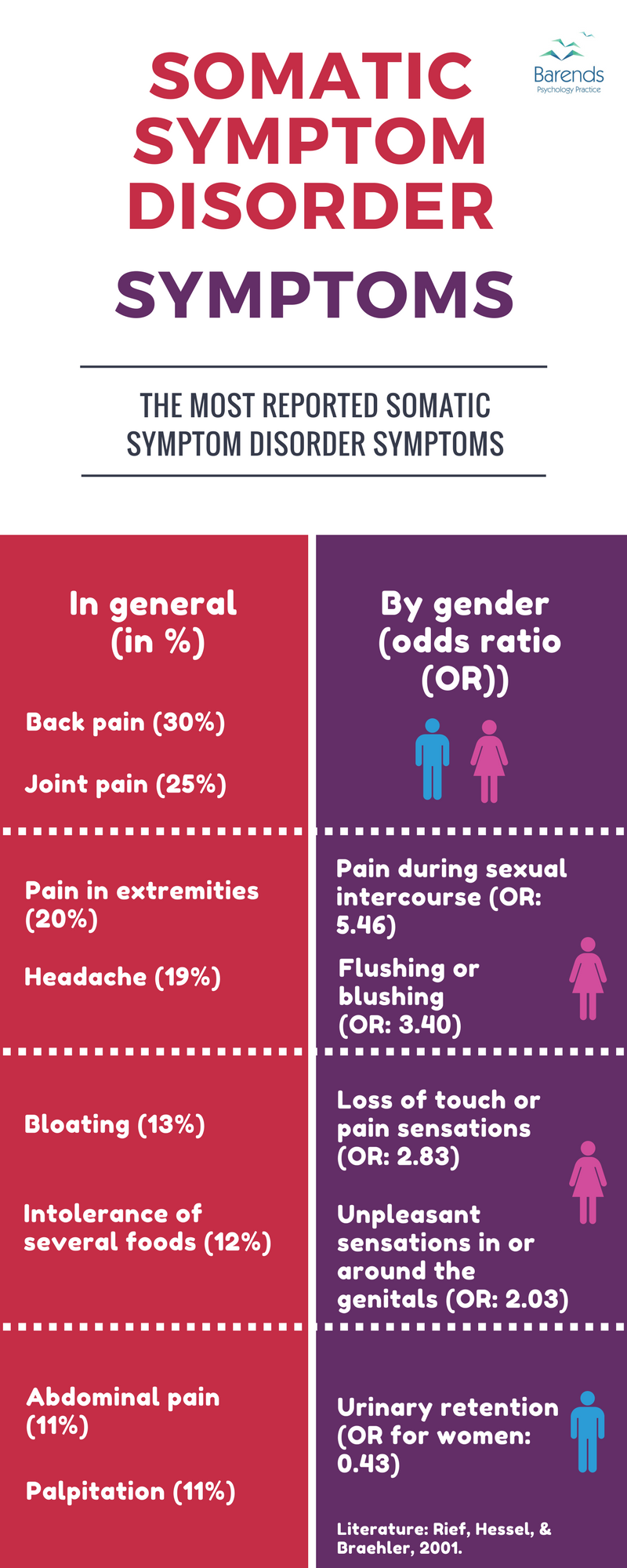
The most reported symptoms for Somatic Symptoms Disorder (SSD) are pain symptoms, followed by gastrointestinal symptoms as well as cardiovascular symptoms [11]. Rare symptoms (only 2% or less of the population reports these) are “rectal pain, pain during intercourse, vomiting, discharge of fluids from anus, unpleasant sensations around the genitals, paralysis and muscle weakness, loss of voice, hallucinations, loss of touch sensations, double vision, blindness, seizures, fainting, or vomiting during whole pregnancy” [11].
Common SSD symptoms [11]:
- Back pain (30% of the respondents reported)
- Joint pain (25%)
- Pain in extremities (20%)
- Headache (19%)
- Bloating (13%)
- Intolerance of several foods (12%)
- Abdominal pain (11%)
- Palpitation (11%)
Somatic Symptom Disorder symptoms significantly reported more often by women [11]:
- Pain during sexual intercourse (Odds Ratio (OR) women: 5.46)
- Flushing or blushing (OR: 3.40)
- Loss of touch or pain sensations (OR: 2.83)
- Unpleasant sensations in or around the genitals (OR: 2.03)
NOTE: Only one symptom is more often reported by men: Urinary retention.
Somatic symptom disorder facts: prevalence in the Netherlands
- In the Netherlands, 16.1% of people has been diagnosed with a Somatic Symptom Disorder (SSD) [2]. This is similar to the 16.2% found in the German population [1].
- People aged 25-44 were more often diagnosed with SSD, compared to the age groups 45-64 and 65 and older: 21.8% versus 15.3% and 5.4% [2].
- Women tend to develop SSD more often than men, but this difference is not significant [2].
- In the Netherlands, of all people with SSD, 26% also had an anxiety and/or depressive disorder [2].
- 54% of the people with an anxiety and/or depressive disorder also had SSD [2].
(Advertisement, please scroll down for more interesting somatic symptoms disorder facts)
Somatic symptom disorder facts: prevalence in Germany
- 5.6% of the German population has been diagnosed with Somatic Symptom Disorder (SSD) at least once in their lives [1].
- In the past 12 months, 4.3% of the German population has been diagnosed with SSD [1].
- More women than men developed SSD in Germany: 7.3% versus 3.9% [1].
- Somatic Symptom Disorder usually develops between adolescence and early adulthood; the median is at the age of 20 [1].
- 12.7% of the German population has been diagnosed with Pain disorder (now known as Conversion Disorder) at least once in their lives [1].
- In the past 12 months, 8.1% has been diagnosed with Pain disorder [1].
- More women than men developed Pain disorder: 17.8% versus 7.8% [1].
- In Germany, 12% of the population was diagnosed with a Somatic Symptom Disorder (SSD) and an anxiety disorder at the same time (comorbidity); 11% with SSD, anxiety disorder, and depressive disorder; 8% with SSD and depressive disorder [1].
- Unlike with other mental disorders, marital status does not correlate significantly with SSD: as many married people develop this disorder as divorced, single or widowed people do [1].
- People in the upper social class developed SSD less often than people from lower social classes [1].
Somatic symptom disorder facts: prevalence in Spain
- 28.8% of the people in Spain who participated in a study had Somatic Symptom Disorder (SSD) [9].
- More women than men were diagnosed with SSD: 71.1% versus 28.9% [9].
- The majority of people with SSD is married (61.6%), followed by never married (16.7%), separated/divorced (11.1%) and widowed (10.6%) [9].
- 18.6% of the people with SSD also had a mood disorder [9].
- Of the people with SSD, 14.8% had an anxiety disorder [9].
- 11.5% of the people with SSD had also a mood disorder and an anxiety disorder [9].
(Advertisement, please scroll down for more interesting somatic symptoms disorder facts)
Somatic symptom disorder facts: prevalence in Saudi Arabia
- In Saudi Arabia, 19.3% of people has been diagnosed with a Somatic Symptoms Disorder (SSD) [8].
- In Saudi Arabia, women are more likely to develop SSD than men: 69.9% versus 30.1% [7].
Somatic symptom disorder facts: treatment
- Cognitive Behavioural Therapy (CBT) is the most effective treatment for Somatic Symptom disorders (SSD) -convulsion disorder and pain disorder were not included in this study- followed by a consultation letter to the primary care physician [4],[12]. Antidepressants were effective as well, but this is not conclusive yet [4].
- As mentioned before, one in two people with SSD report childhood traumatization by a primary caregiver, which suggests that EMDR may be beneficial for those suffering from SSD. Preliminary evidence suggests that, indeed, EMDR is effective in reducing chronic pains, especially when someone with SSD experienced something traumatic in their childhood [13]. EMDR has also been effective in treating phantom limb pain and the psychological consequences of amputation [14].
- At least 32.9% of the people with SSD received treatment for their disorder. For people with SSD had another mental disorder this was 47.7% [1].
- At least 25.0% of the people with Pain disorder received treatment for their disorder. For people with Pain disorder had another mental disorder this was 35.6% [1].
- A good support network reduces the amount of stress perceived someone with somatic symptom disorder, which improves the quality of life significantly [16]
- Patients with severe somatic symptom disorder have twice the annual medical care costs of nonsomatizing patients. Also, they have twice the outpatient and inpatient medical care utilization [15].
Literature:
- [1] Jacobi, F., Wittchen, H. U., Hölting, C., Höfler, M., Pfister, H., Müller, N., & Lieb, R. (2004). Prevalence, co-morbidity and correlates of mental disorders in the general population: results from the German Health Interview and Examination Survey (GHS). Psychological medicine, 34, 597-611.
- [2] De Waal, M. W., Arnold, I. A., Eekhof, J. A., & Van Hemert, A. M. (2004). Somatoform disorders in general
practice. The British Journal of Psychiatry, 184, 470-476. - [3] Pauli, P., & Alpers, G. W. (2002). Memory bias in patients with hypochondriasis and somatoform pain disorder. Journal of Psychosomatic Research, 52, 45-53.
- [4] Kroenke, K. (2007). Efficacy of treatment for somatoform disorders: a review of randomized controlled trials. Psychosomatic medicine, 69, 881-888.
- [5] van Dijke, A., Ford, J. D., van der Hart, O., van Son, M., van der Heijden, P., & Bühring, M. (2010). Affect dysregulation in borderline personality disorder and somatoform disorder: Differentiating under-and over-regulation. Journal of Personality Disorders, 24, 296-311.
- [6] Annemiek van, D., Julian D, F., Onno van der, H., Maarten JM, V. S., Peter GM, V. D. H., & Martina, B. (2011). Childhood traumatization by primary caretaker and affect dysregulation in patients with borderline personality disorder and somatoform disorder. European Journal of Psychotraumatology, 2, 5628.
- [7] Marshall, T., Jones, D. P., Ramchandani, P. G., Stein, A., & Bass, C. (2007). Intergenerational transmission of health beliefs in somatoform disorders. The British Journal of Psychiatry, 191, 449-450.
- [8] Becker, S., Al Zaid, K., & Al Faris, E. (2002). Screening for somatization and depression in Saudi Arabia: a validation study of the PHQ in primary care. The International Journal of Psychiatry in Medicine, 32, 271-283.
- [9] Roca, M., Gili, M., Garcia-Garcia, M., Salva, J., Vives, M., Campayo, J. G., & Comas, A. (2009). Prevalence and comorbidity of common mental disorders in primary care. Journal of affective disorders, 119, 52-58.
- [10] Härter, M., Baumeister, H., Reuter, K., Jacobi, F., Höfler, M., Bengel, J., & Wittchen, H. U. (2007). Increased 12-month prevalence rates of mental disorders in patients with chronic somatic diseases. Psychotherapy and psychosomatics, 76, 354-360.
- [11] Rief, W., Hessel, A., & Braehler, E. (2001). Somatization symptoms and hypochondriacal features in the general population. Psychosomatic medicine, 63, 595-602.
- [12] Sumathipala, A. (2007). What is the evidence for the efficacy of treatments for somatoform disorders? A critical review of previous intervention studies. Psychosomatic medicine, 69, 889-900.
- [13] van Rood, Y. R., & de Roos, C. (2009). EMDR in the treatment of medically unexplained symptoms: A systematic review. Journal of EMDR Practice and Research, 3, 248-263.
- [14] Schneider, J., Hofmann, A., Rost, C., & Shapiro, F. (2007). EMDR in the treatment of chronic phantom limb pain. Pain Medicine, 9, 76-82.
- [15] Barsky, A. J., Orav, E. J., & Bates, D. W. (2005). Somatization increases medical utilization and costs independent of psychiatric and medical comorbidity. Archives of general psychiatry, 62, 903-910.
- [16] Ali, A., Deuri, S. P., Deuri, S. K., Jahan, M., Singh, A. R., & Verma, A. N. (2010). Perceived social support and life satisfaction in persons with somatization disorder. Industrial psychiatry journal, 19, 115.