
Treating Depression: which treatments and medication?
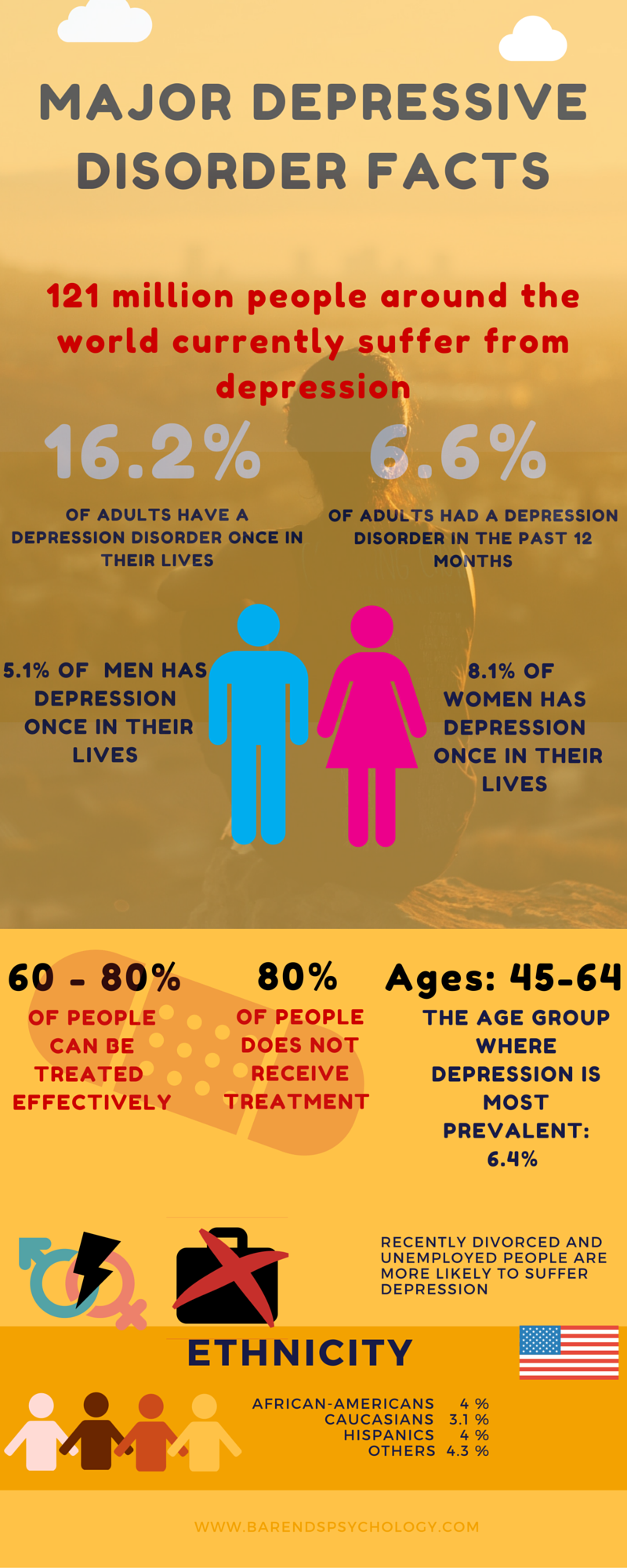
Major depression facts – infographic.
Treating depression is effective in at least 60% of the cases. A mental health professional can treat depression using psychotherapy, medication or a combination of both. A combination of therapy and medication is the most effective one, because the depressed person feels a lot better due to the medication and that can positively affect the psychotherapy progress. Medication alone, however, usually is not as effective on the long run. It’s important that someone learns how to prevent himself or herself from relapsing. On this page you find more information about treating depression.
- What is depression?
- Depression causes.
- How is depression diagnosed?
- How can I cope with depression myself?
- Online depression test.
- Interesting depression facts.
- Online counseling for depression.
- Take me to the homepage.
At Barends Psychology Practice, we treat various types of depression. Interested? Make an appointment for a free first session now! Go to contact us. (Depending on your health insurance, sometimes treatment can be reimbursed).
Both cognitive behavioural therapy and medication (also combined) are effective in treating depression. A doctor or psychiatrist is authorized to write prescriptions like antidepressants, but be aware that the effectiveness of medication differs per patient. Always check with a doctor or psychiatrist which medication works the best for treating depression. According to research, treating depression using cognitive behavioural therapy may even be a better choice. At Barends Psychology Practice, we offer online counseling for treating depression using cognitive behavioural therapy and acceptance and commitment therapy.
After termination of treatment (medication and/or cognitive behavioural therapy) depression may return over time. However, recent research indicates that someone who had cognitive behavioural therapy (focused on cognitions, fantasies and day dreaming) is better protected against a relapse.
A brief overview of effective treatment options:
Treating depression with Cognitive Behavioural Therapy
According to the theory of Cognitive Behavioural Therapy, a person’s mood is directly related to his or her thought patterns. A person’s mood, sense of self, physical state and behaviour is affected by negative, dysfunctional thinking. Cognitive behavioural therapy’s goal is to help a person to learn to recognize negative thought patterns, evaluate their validity, and replace them with healthier and more realistic ways of thinking. Also cognitive behavioural therapists aim to change behaviour patterns resulting from negative, dysfunctional thinking. We believe that negative, dysfunctional thinking results in negative, dysfunctional behaviour which results in negative, dysfunctional thinking (a downward spiral). By changing these patterns, research shows, the mood changes as well.
Cognitive behavioural therapy is effective in treating depression (non-chronic), such as light to mild depression. Online counseling is based on cognitive behavioural therapy and is proven to be effective in treating depression.
Acceptance and Commitment Therapy is a form of cognitive behavioural therapy and effective in treating depression as well. Acceptance and commitment therapy’s theory suggests that people get depressed due to the need for control over feelings, thoughts, memories and physical sensations. This need for control, according to the acceptance and commitment theory, may lead to avoidance of certain normal experiences, like fear, anxiety, loneliness and sadness. This need for control may also lead to the feeling of ‘being trapped in one’s own thoughts’, making it almost impossible to enjoy life. Acceptance and commitment therapy focuses on the above mentioned processes and helps the patient to accept that all experiences are part of life, not only the pleasant thoughts, feelings and memories.
(Advertisement. For more information, please scroll down.)
Treating depression with medication – Antidepressants
Selective serotonin-reuptake inhibitors (SSRI): In people with depression neurotransmitters do not work efficient enough, because they are reabsorbed too quickly after being released. SSRIs inhibit the re-uptake of the neurotransmitter serotonin allowing serotonin to be active for a longer period of time. Serotonin affects sleep, mood and appetite. Free slot games with bonus rounds no download no registration at https://reallybestslots.com/slots-online/ play now in demo video slots with enjoy Side effects could be: sleeplessness, nausea, decreased appetite, sexual problems and constipation.
Effectiveness: Two meta-analyses published in 2008 (Kirsch) and 2010 (Fournier) found in people with mild and moderate depression that the effect of SSRIs is small to none compared to placebo, while in severe depression the effect was found to be relatively small to substantial. Also in short term mild depression antidepressants had no advantage over placebo (source: NICE review). Treating depression using SSRIs may be effective for some people, but as research suggests, SSRIs are probably not the best choice in treating depression.
Selective serotonin-norepinephrine re-uptake inhibitors (SNRI): SNRI does not only inhibits the re-uptake of serotonin but also of norepinephrine. Some SNRIs even inhibit the re-uptake of dopamine. SSRIs and SNRIs work nearly identical. Currently research focuses on when to prescribe SSRIs or SNRIs. Side effects of SNRIs are: sleepiness, hypertension, gastrointestinal symptoms, weight gain or loss, restlessness, tremors, yawning, sedation, insomnia, and sexual dysfunction (abnormal erection and ejaculation, decreased libido).
Effectiveness: data from clinical trials suggest that SNRIs are more effective than SSRIs in treating depression and come with less side effects. Even though treating depression with CBT may still be more effective (research suggests), SNRIs may be a good alternative to that.
(Advertisement. For more information, please scroll down.)
Monoamine Oxidase Inhibitors (MAOI): MAOIs inhibit the activity of the monoamine oxidase enzyme family. Mono-amines regulate blood pressure, mood and movement. Examples of mono-amines are neurotransmitters norepinephrine, adrenaline, dopamine and serotonin. Classical MAOIs are hardly used because they are dangerous in combination with cheese, sauerkraut and beer. Modern MAOIs are more selective and conventional than classic MAOIs. Two types of modern MAOIs: MAO-A and MAO-B. MAO-A provides in an anti-depressive effect. MAO-B is used in Parkinson’s disease.
Effectiveness: MAOIs have found to be effective in treating atypical depression, depression and are very effective in treating bipolar depression. Depending on the depression type using MAOIs can be very effective in treating depression.
Tricyclic antidepressants (TCAs): Tricyclic antidepressants inhibit the reuptake of the neurotransmitters serotonin and norepinephrine, causing serotonin and norepinephrine to be longer available in the brains. It takes TCAs a few weeks to start working, because the right balance must be ‘built up’ in the blood. Fifty to sixty percent of the adults responds well to TCAs. Side effects of TCAs: dry mouth, constipation, bladder problems, sexual dysfunction, dizziness and increased heart rate. In other words: Treating depression using TCAs is effective in slightly more than half of all the patients.