
Somatic Symptom Disorder Treatment Options
Written by Niels Barends, MSc, psychologist with more than 14 years of clinical experience treating trauma, anxiety disorders, emotional dysregulation, and somatic symptom disorder. Updated May 2026.
Somatic symptom disorder treatment focuses on reducing distress connected to physical symptoms, improving emotional regulation, decreasing fear and body monitoring, and helping people regain daily functioning and quality of life.
People with somatic symptom disorder (SSD) often experience persistent physical symptoms such as pain, dizziness, gastrointestinal complaints, fatigue, or other bodily sensations that become strongly connected to anxiety, stress, fear, or emotional distress. Effective treatment helps reduce the cycle of symptom monitoring, reassurance seeking, avoidance, and catastrophic interpretations of bodily sensations.
In clinical practice, somatic symptom disorder may overlap with anxiety disorders, complex PTSD, panic symptoms, depression, or emotional dysregulation patterns seen in conditions such as borderline personality disorder. Treatment therefore often needs to address both physical symptom distress and underlying emotional or trauma-related patterns.
Research support is strongest for cognitive behavioural therapy (CBT), while psychodynamic interpersonal psychotherapy and trauma-focused approaches such as EMDR may be helpful for some people, especially when emotional conflict or trauma contributes to the symptoms [2],[3],[4],[11],[13].
Key facts about somatic symptom disorder treatment
- CBT is currently the most researched treatment for somatic symptom disorder.
- Treatment often focuses on reducing body monitoring, reassurance seeking, fear, and avoidance behaviors.
- EMDR may help when symptoms are linked to trauma or unresolved emotional experiences.
- Psychodynamic therapy may improve emotional awareness and reduce symptom-focused rumination.
- Many evidence-based approaches used for somatic symptom disorder, including CBT and trauma-focused therapy, can also be delivered online when clinically appropriate.
- Treatment is usually most effective when psychological and physical aspects are addressed together.
— Niels Barends, MSc, psychologist at Barends Psychology Practice
Somatic symptom disorder treatment guide
Need help with somatic symptom disorder?
If physical symptoms, health anxiety, or body-related fear are disrupting your life, therapy can help reduce distress and improve emotional and physical functioning.
Not sure whether your symptoms may fit somatic symptom disorder? You can also take our online somatic symptom disorder test for a first indication.
Somatic symptom disorder treatment – Cognitive Behavioural Therapy (CBT)
Cognitive behavioural therapy (CBT) is currently one of the most researched and effective treatments for somatic symptom disorder [2],[3]. CBT has been shown to reduce somatic symptoms, decrease health-related anxiety, and improve daily functioning, including in older adults [8],[10].
Treatment usually focuses on reducing catastrophic interpretations of bodily sensations, decreasing reassurance seeking, reducing body monitoring, improving stress regulation, and rebuilding confidence in normal activities.
Many people with SSD become trapped in cycles of symptom checking, fear, avoidance, and physical tension. CBT helps interrupt these cycles and teaches people to respond to bodily sensations in a less threatening and more balanced way. Some of these practical strategies are also discussed on our page about coping with somatic symptom disorder.
Some CBT-based approaches also integrate mindfulness techniques. Mindfulness-based therapies may help people observe physical sensations with less fear or judgment, although traditional CBT currently has stronger research support [9].
Somatic symptom disorder treatment – Psychodynamic interpersonal psychotherapy (PIT)
Psychodynamic interpersonal psychotherapy (PIT) may also help people with persistent somatic symptoms, particularly when emotional conflicts, relationship difficulties, or earlier life experiences contribute to symptom patterns [11],[12].
PIT focuses on increasing emotional awareness, reducing rumination, improving bodily relaxation, and understanding connections between emotional experiences and physical symptoms.
Some individuals with somatic symptom disorder have difficulty identifying or expressing emotional distress directly. In these cases, emotions may become more strongly expressed through physical symptoms. Psychodynamic therapy may help people better understand these patterns and improve emotional processing.
Although PIT can improve quality of life and reduce somatic symptoms, CBT currently has stronger overall evidence for treating somatic symptom disorder [2],[3].
Somatic symptom disorder treatment – EMDR therapy
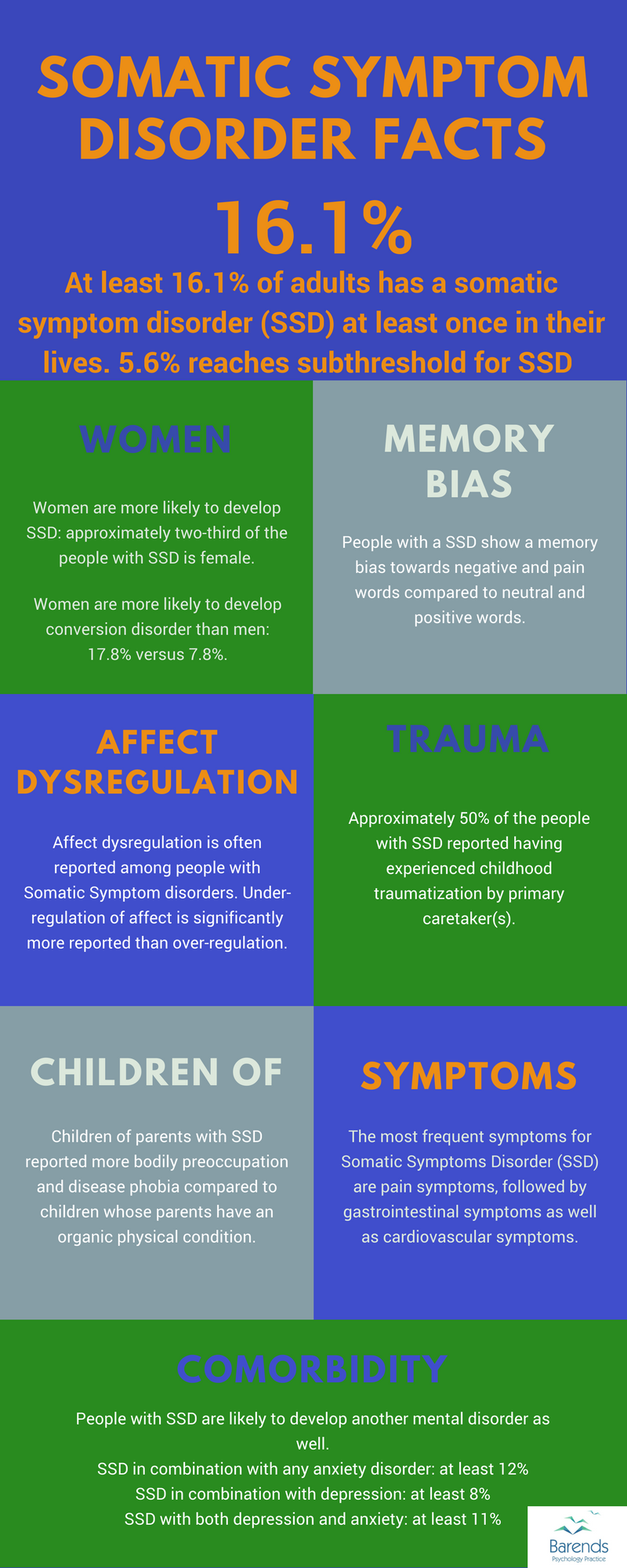
Research suggests that trauma may play an important role in somatic symptom disorder for some individuals. One study found that approximately 50% of people with somatic symptom disorder reported childhood traumatization by a primary caregiver [14].
Because trauma can increase nervous system sensitivity and body-based threat responses, trauma-focused therapies such as EMDR therapy may help reduce somatic symptoms when unresolved traumatic experiences contribute to the symptom pattern.
Research suggests that EMDR may reduce chronic pain, medically unexplained symptoms, and trauma-related physical distress [4],[5],[13]. Some studies also found improvements in depression symptoms and overall emotional functioning [13].
EMDR focuses on processing unresolved memories, emotional experiences, and body-based fear responses that may continue to activate the nervous system long after the original experiences occurred.
For people with trauma histories, emotional dysregulation, or conditions such as borderline personality disorder, addressing trauma-related stress patterns may be an important part of treatment.
Medication for somatic symptom disorder
Medication may help some individuals with somatic symptom disorder, particularly when symptoms overlap with anxiety disorders or depression. However, research on medication for SSD remains limited and mixed [2].
Medication alone is usually not considered the most effective long-term treatment approach. In most cases, therapy remains central because treatment often requires changing how physical sensations are interpreted, monitored, and emotionally processed.
Online therapy for somatic symptom disorder
Online therapy can be an effective treatment option for somatic symptom disorder. Many evidence-based therapies, including CBT and trauma-focused therapy, can be provided effectively through online sessions.
Online treatment may be particularly useful for people who experience high anxiety, chronic stress, physical exhaustion, or difficulties leaving home because of health-related fears or physical symptoms.
When to seek professional help
It may be helpful to seek professional support if physical symptoms are causing significant distress, repeated medical reassurance seeking, anxiety, avoidance, or disruptions in work, relationships, sleep, or daily functioning.
Professional support can help determine whether symptoms fit somatic symptom disorder, health anxiety, trauma-related symptoms, panic symptoms, or another condition. Treatment can also help reduce fear around bodily sensations and improve overall quality of life.
Struggling with physical symptoms, health anxiety, or chronic stress?
Treatment can help reduce fear around bodily sensations and improve emotional and physical functioning.
Frequently asked questions about somatic symptom disorder treatment
What is the best treatment for somatic symptom disorder?
CBT is currently the most researched treatment for somatic symptom disorder. Trauma-focused approaches and psychodynamic therapy may also help, depending on the underlying causes and symptom patterns.
Can trauma therapy help somatic symptoms?
Yes. Trauma-focused therapies such as EMDR may help when physical symptoms are connected to unresolved trauma, chronic stress, or nervous system hyperactivation.
Can somatic symptom disorder be treated online?
Yes. Online therapy can effectively provide CBT, EMDR, and other evidence-based treatments for somatic symptom disorder.
How long does treatment usually take?
Treatment duration varies depending on symptom severity, trauma history, emotional regulation difficulties, and overlapping mental health conditions. Some people improve within several months, while others benefit from longer-term support.
Is medication enough to treat somatic symptom disorder?
Medication may help reduce anxiety or depressive symptoms, but therapy is usually important because treatment often involves changing patterns of fear, avoidance, and body monitoring.
