
Acute Stress Disorder Facts and Diagnosis According to the DSM-5
Acute stress disorder facts
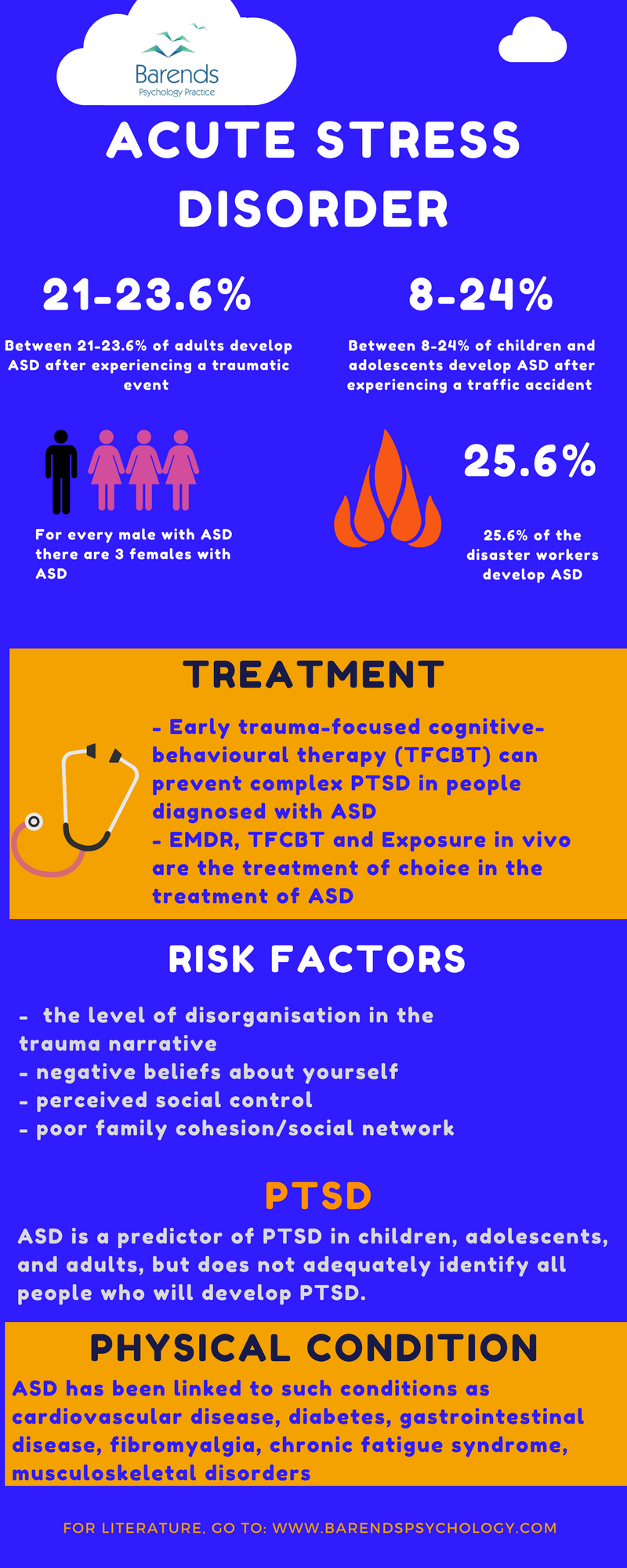
A proper acute stress disorder (ASD) diagnosis is essential for individuals to receive effective professional treatment for their mental health condition. Early intervention shortly after a traumatic event reduces ASD symptoms and lowers the risk of developing PTSD within a month [1][2]. Additionally, timely treatment significantly improves the overall quality of life for those affected [3]. Professionals diagnose ASD by using specific questionnaires and conducting interviews based on the DSM-5 or ICD-10 criteria. Once diagnosed, a tailored treatment plan can address the individual’s unique needs. This page outlines the official criteria for diagnosing ASD, provides explanations, and includes examples to clarify the requirements. The criteria come from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), published by the American Psychiatric Association.
If you would like a therapist to help you with these issues, you can book a free, no-obligation consultation with us here.
Go to:
- What is ASD?
- What causes ASD?
- ASD treatment.
- How to cope with ASD.
- Helping your partner with ASD.
- Take the ASD test.
- ASD facts.
- Online counseling for ASD.
- Take me to the homepage.
At Barends Psychology Practice, acute stress disorder treatment is offered. Go to contact us to schedule a first, free session.
Acute stress disorder diagnosis – Criterion 1
The first criterion addresses how an individual experienced the traumatic event. To meet this criterion, the person must have been exposed to:
Exposure can occur in any of the following ways (only one is required to fulfill the criterion):
Acute Stress Disorder Diagnosis – Criterion 1: Examples
- Direct exposure: Being in a car accident.
- Witnessing the trauma: Observing a traffic accident as it occurs.
- Indirect exposure (close friend or relative): Learning that your best friend was involved in a serious car accident.
- Repeated or extreme indirect exposure to aversive details: A first responder performing CPR on a traffic accident victim.
Acute Stress Disorder Diagnosis – Criterion 2
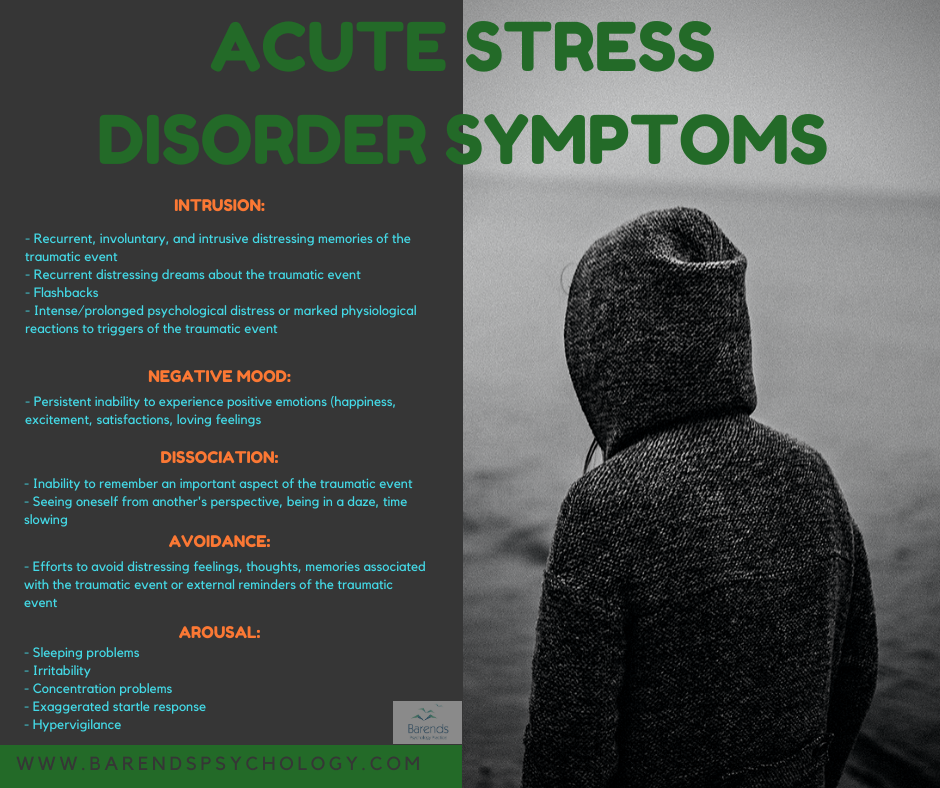
Intrusion Symptoms:
- Recurrent, involuntary, and intrusive distressing memories of the traumatic event.
- Recurrent distressing dreams related to the event. • Example: Having nightmares about the person who assaulted you.
- Dissociative reactions (e.g., flashbacks) where the individual feels the traumatic event is recurring.
- Intense or prolonged psychological distress or strong physical reactions to triggers that resemble the traumatic event.
- Example: Watching a robbery on television could trigger hyperventilation or trembling if the person recently experienced a robbery.
- Note: Children may express themes of the trauma through repetitive play or experience nightmares unrelated to the event.
Negative mood:
- Persistent inability to feel positive emotions, such as happiness, joy, or love.
Dissociative symptoms:
- An altered sense of reality regarding one’s surroundings or oneself. • Example: Feeling detached, seeing oneself from another’s perspective, or experiencing a slowing of time.
- Inability to remember important aspects of the traumatic event due to dissociative amnesia. • Example: Forgetting the first few minutes following a car accident, unrelated to head injury or substance use.
Avoidance symptoms:
- Avoiding distressing memories, thoughts, or feelings about the traumatic event. • Example: Using alcohol or drugs to suppress memories of the event.
- Avoiding external reminders (people, places, conversations, etc.) linked to the trauma. • Example: Avoiding the city center after being mugged there at night.
Arousal symptoms:
- Difficulty falling or staying asleep, or restlessness during sleep.
- Irritable behavior or angry outbursts with little or no provocation, expressed as verbal or physical aggression.
- Hypervigilance.
- Problems concentrating.
- Exaggerated startle response.
Acute stress disorder diagnosis – Criterion 3
The symptoms must persist for a duration of 3 days to 1 month after the trauma. While some symptoms may appear immediately after the event, they must last at least 3 days to meet this criterion. If symptoms persist beyond one month, the diagnosis may shift to Post-Traumatic Stress Disorder (PTSD).
Acute stress disorder diagnosis – Criterion 4
The symptoms must cause significant distress or impair the individual’s ability to function in social, occupational, or other important areas of life.
(Advertisement. For more information about ASD, please scroll down).
Acute stress disorder diagnosis – Criterion 5
The disturbance cannot be attributed to the effects of substances (e.g., medication or alcohol), another medical condition (e.g., mild traumatic brain injury), or a different diagnosis such as brief psychotic disorder.
Literature
- [1] Ponniah, K., & Hollon, S. D. (2009). Empirically supported psychological treatments for adult acute stress disorder and posttraumatic stress disorder: a review. Depression and anxiety, 26, 1086-1109.
- [2] Kornør, H., Winje, D., Ekeberg, Ø., Weisæth, L., Kirkehei, I., Johansen, K., & Steiro, A. (2008). Early trauma-focused cognitive-behavioural therapy to prevent chronic post-traumatic stress disorder and related symptoms: a systematic review and meta-analysis. BMC psychiatry, 8, 81.
- [3] Holbrook, T. L., Hoyt, D. B., Coimbra, R., Potenza, B., Sise, M., & Anderson, J. P. (2005). High rates of acute stress disorder impact quality-of-life outcomes in injured adolescents: mechanism and gender predict acute stress disorder risk. Journal of Trauma and Acute Care Surgery, 59, 1126-1130.