
Why Is a Borderline Personality Disorder Diagnosis Important?
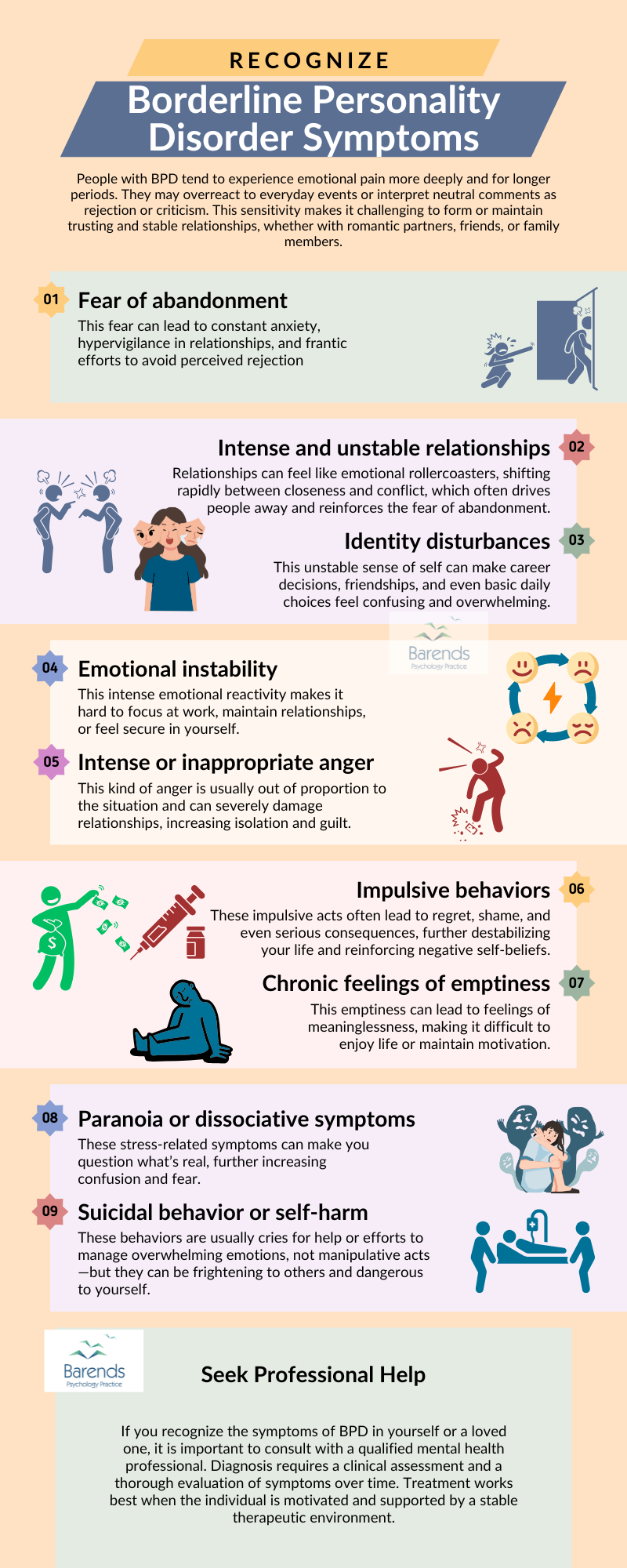
Borderline personality disorder symptoms.
A borderline personality disorder diagnosis is crucial for identifying the right treatment. People with borderline personality disorder (BPD) often experience an extreme fear of abandonment and have difficulty regulating emotions. This can result in impulsive and unstable behavior, severe mood swings, intense and chaotic relationships, and low self-esteem.
Individually, these symptoms could point to other mental health conditions. For instance:
- Fear of abandonment may relate to post-traumatic stress disorder (PTSD),
- Severe mood swings could suggest bipolar disorder,
- Low self-esteem might be linked to depression or anxiety.
However, when these features cluster together, they strongly indicate borderline personality disorder. A clear diagnosis allows professionals to offer the most effective treatments and tailor support to the patient’s specific needs.
Borderline Personality Disorder – Easy and quick explanation of the BPD symptoms and the differences between DSM-5-TR and ICD-11!
Why a Formal Diagnosis Matters
Effective treatment begins with accurate diagnosis. Research shows that Schema Therapy and Dialectical Behavior Therapy (DBT) are the most effective treatments for BPD [1],[2]. But these approaches work best when applied to patients who meet the diagnostic criteria for BPD.
A treatment is considered effective when it reduces disorder-specific symptoms both in the short and long term. Therefore, knowing whether someone meets the BPD diagnosis criteria is essential for choosing the most appropriate treatment strategy. Without a diagnosis, the risk of misdiagnosis and ineffective treatment increases significantly.
At Barends Psychology Practice, we offer online therapy for borderline personality disorder. Contact us today to schedule your first online session, free of charge.
Jump to:
- What is borderline personality disorder?
- BPD symptoms explained
- What causes people to develop borderline?
- What are the treatment options for borderline?
- Borderline personality disorder test.
- Coping with BPD yourself.
- Living with someone who has BPD.
- Interesting borderline personality disorder facts.
- Online counseling for Borderline personality disorder.
- Take me to the homepage.
Borderline personality disorder diagnosis according to the DSM-5-TR
According to the DSM-5-TR (Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision), BPD is diagnosed based on impairments in personality functioning and pathological personality traits.
(A) – Significant impairments in personality functioning manifest by:
- 1. Impairments in self-functioning (a or b):
a) Identity: markedly impoverished, poorly developed, or unstable self-image, often associated with excessive self-criticism; chronic feelings of emptiness; dissociative states under stress.
b) Self-direction: Instability in goals, aspiration, values, or career plans.
AND
- 2. Impairments in interpersonal functioning (a or b):
a) Empathy: Compromised ability to recognize the feelings and needs of others associated with interpersonal hypersensitivity (i.e., prone to feel slighted or insulted); perceptions of others selectively biased toward negative attributes or vulnerabilities.
b) Intimacy: Intense, unstable, and conflicted close relationships, marked by mistrust, neediness, and anxious preoccupation with real or imagined abandonment; close relationships often viewed in extremes of idealization and devaluation and alternating between over involvement and withdrawal.
(B). Pathological personality traits in the following domains:
- 1. Negative Affectivity, characterized by:
a) Emotional liability: unstable emotional experiences and frequent mood changes; emotions that are easily aroused, intense, and/or out of proportion to events and circumstances.
b) Anxiousness: intense feelings of nervousness, tenseness, or panic, often in reaction to interpersonal stresses; worry about the negative effects of past unpleasant experiences and future negative possibilities; feeling fearful, apprehensive, or threatened by uncertainty; fears of falling apart or losing control.
c) Separation insecurity: Fears of rejection by -and/or separation from- significant others, associated with fears of excessive dependency and complete loss of autonomy.
d) Depressivity: Frequent feelings of being down, miserable, and/or hopeless; difficulty recovering from such moods; pessimism about the future; pervasive shame; feeling of inferior self-worth; thoughts of suicide and suicidal behaviour.
(Advertisement. For more information, please scroll down.)
- 2. Disinhibition, characterized by:
a) Impulsiveness: acting on the spur of the moment in response to immediate stimuli; acting on a momentary basis without a plan or consideration of outcomes; difficulty establishing or following plans; a sense of urgency and self-harming behaviour under emotional distress.
b) Risk taking: engagement in dangerous, risky, and potentially self-damaging activities; unnecessarily and without regard to consequences; lack of concern for one’s limitations and denial of the reality of personal danger. - 3. Antagonism, characterized by:
a) Hostility: persistent or frequent angry feelings; anger or irritability in response to minor insights and insults.
(C). The impairments in personality in functioning and the individual’s personality trait expression are relatively stable across time and consistent across situations.
(D). The impairments in personality functioning and the individual’s personality trait expression are not better understood as normative for the individual’s developmental stage or socio-cultural environment.
(E). The impairments in personality functioning and the individual’s personality trait expression are not solely due to the direct physiological effects of a substance (e.g.: a drug of abuse, medication) or a general medical condition (e.g.: severe head trauma).
(Advertisement. For more information, please scroll down.)
Borderline personality disorder diagnosis According to the ICD-11
The ICD-11 (International Classification of Diseases, 11th Edition) approaches personality disorders differently. Instead of listing specific disorders, it describes severity levels and prominent trait domains, then allows optional specification of subtypes such as Borderline Pattern.
To meet the ICD-11 Borderline Pattern specification, a person must be diagnosed with a personality disorder and exhibit at least five of the following features:
1. Marked impulsivity
Definition: Difficulty delaying gratification; acting without considering consequences, especially when distressed.
Example: Spending large amounts of money, engaging in unsafe sex, binge eating, or reckless driving after an argument or emotional trigger.
2. Severely unstable relationships
Definition: Intense, chaotic, and quickly shifting interpersonal relationships that often alternate between idealization and devaluation.
Example: A person may adore a partner one day and block or insult them the next, based on perceived rejection or criticism.
3. Fear of abandonment
Definition: Extreme sensitivity to perceived or real signs of rejection or separation.
Example: Feeling panicked or furious when a loved one is late or doesn’t reply to a message quickly. This may lead to desperate attempts to keep them close, such as threatening self-harm or begging.
4. Emotional instability due to reactivity
Definition: Rapid and intense emotional responses to interpersonal events.
Example: Becoming severely depressed or enraged for hours after a minor disagreement or slight.
5. Chronic feelings of emptiness
Definition: A persistent internal void or sense of nothingness that is not situational.
Example: Despite being surrounded by people or involved in activities, the person feels numb, hollow, or disconnected from themselves or others.
6. Poor self-image or unstable sense of self
Definition: A fluctuating or unclear sense of identity, goals, values, or self-worth.
Example: The person may one day feel confident and ambitious, and the next feel worthless, directionless, or unsure of who they are.
7. Intense or poorly controlled anger
Definition: Difficulty managing anger, often disproportionate to the situation, and sometimes explosive.
Example: Overreacting with rage to mild criticism, yelling or becoming physically aggressive when feeling misunderstood or slighted.
8. Stress-related paranoia or dissociation
Definition: Under extreme stress, a person may experience brief paranoid thoughts or feel emotionally numb and disconnected (dissociation).
Example: Feeling as though the world isn’t real (derealization), or watching oneself from outside the body (depersonalization), often after conflict or emotional overload.
9. Suicidal behavior or self-harm
Definition: Recurrent thoughts of suicide, suicide attempts, or deliberate self-injury (e.g., cutting, burning) without suicidal intent, often to regulate emotional pain.
Example: After an argument or intense feelings of rejection, a person may cut themselves to feel relief or regain a sense of control.
(Advertisement. For more information, please scroll down.)
DSM-5-TR vs ICD-11: Key Differences
Structure
Focus
Diagnosis
Severity Assessment
Utility
Categorical + dimensional hybrid model
Specific diagnostic criteria for BPD
Requires specific traits + impairments
Optional (Alternative Model in Section III)
Commonly used in the U.S. and parts of Europe
Fully dimensional model
Broad personality disorder + optional “Borderline Pattern”
Requires general PD + 5/9 borderline traits
Required (Mild / Moderate / Severe)
WHO standard, used worldwide
In practice: Both systems aim to capture the same core features of BPD, but the ICD-11 offers more flexibility and focuses on severity and traits, while DSM-5-TR emphasizes specific symptom clusters.
Get the Right Diagnosis – Start Therapy Today
At Barends Psychology Practice, we specialize in diagnosing and treating BPD using both DSM-5 and ICD-11 frameworks. Understanding how symptoms fit these criteria helps us tailor therapy—whether online or in person—to your specific needs.Contact us today to schedule your first online session, free of charge.
Literature:
12-month, randomised clinical trial in The Netherlands. The British Journal of Psychiatry, 182, 135-140.